Patient Education
-
- Achilles Tendonitis
- Ankle Equinus
- Arthritis of Big Toe joint
- Bunion
- Callus
- Capsulitis
- Flatfoot: Acq'd. PTTD
- Ganglion cysts
- Gouty Arthritis
- Hallux Varus
- Hammertoe deformity
- Ingrown toenails
- Kohler’s Osteochondroses
- Limb Length Inequality
- Metatarsal Arthralgia
- Metatarsal Stress Fracture
- Neuroma - Intermetatarsal
- Pediatric Flat Foot
- Peroneal dislocation
- Peroneal tendon tear
- Plantar Fasciitis
- Plantar Fibroma
- Retrocalcaneal Bursitis
- Sesamoid Fracture
- Shin Splints
- Tarsal Tunnel Syndrome
- Tailor's bunion
- Toenail Fungus
- Warts - Verruca Plantaris
-
- Overview
- Diabetic Shoes
- Shoe Modification
- Accommodative Orthotics
- Ankle Foot Orthosis (AFO) - Overview
- Richie Brace® - AFO
- Dorsiflexory Assist Device (Allard® ToeOFF Brace)
- Gauntlet AFO (Arizona®)
-
- Overview
- Preoperative Care
- Day of Surgery
- Postoperative Care
- Bunionectomy
- Bunionectomy - Post-Op
- Neuroma Surgical Care
- No Barefoot Walking
- Activity Limitations
-
-
-
-
-
Tarsal Tunnel Syndrome
Tarsal tunnel syndrome is a painful entrapment neuropathy involving the posterior tibial nerve as it enters the foot. The term entrapment neuropathy denotes injury to a nerve from an external source. Examples of an entrapment neuropathy could include sciatica symptoms of low back pain originating from an injured disc in the back region that is putting pressure on the nerve root from the spinal cord. Another example would include carpal tunnel syndrome which is hand and wrist pain associated oftentimes with overuse leading to inflammation of the nerves at the wrist level.
Tarsal tunnel, like carpal tunnel is pain associated with injury and inflammation to the posterior tibial nerve as it enters the foot. Symptoms associated with tarsal tunnel syndrome include pain with descriptions of “knife like”, “sharp lancinating” or “numbness” involving the bottom of the foot. The pain is typically minimal in the morning but intensifies during the day’s activity and is not generally associated with swelling of the foot or ankle.
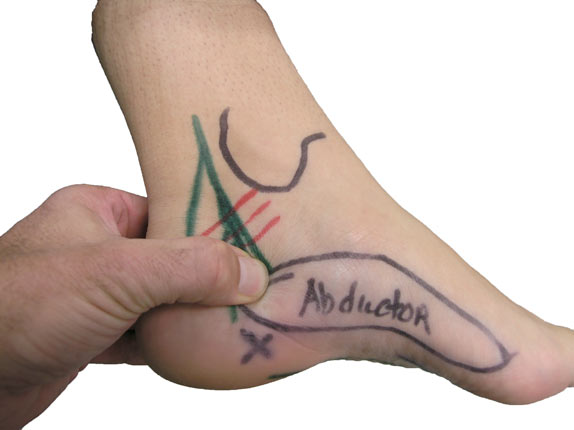
The anatomy of the tarsal tunnel includes the posterior tibial nerve running along the same course as the posterior tibial artery and vein and the long flexor tendons that insert to various areas on the bottom of the foot. The tarsal tunnel region has a floor which is the bony architecture of the foot and ankle and is covered by a strong ligament called the flexor retinaculum. The nerve enters the foot at the porta pedis which is a canal that is formed by the abductor hallucis brevis which is a small muscle on the inside of the foot. It is the region of the porta pedis that the nerve entrapment will usually occur.
Causes of tarsal tunnel are diverse, including; abnormal pressure placed on the nerve from scar tissue occurring from direct nerve trauma, varicose veins, soft tissue masses, thickening or hypertrophy of the small muscles of the foot at the region of the tarsal tunnel and biomechanical instability including abnormal foot pronation.
Tarsal tunnel oftentimes is found in conjunction with a form of heel pain called plantar fascitis. Plantar fascitis is the most common cause of adult heel pain. The pain originates on the bottom of the heel at the attachment site of the plantar fascia. Pain is most noticeable after initial rising from a non-weight-bearing setting. Patients having plantar fascitis that is resistant to conservative treatment may sometimes have pain to clinical exam on the inside of the ankle at the level of the posterior tibial nerve and its branches that are found on the medial portion of the heel bone. The link between the development of plantar fascitis and tarsal tunnel syndrome is not fully understood and could be related to chronic inflammation at the heel level with plantar fascitis and extension of inflammatory changes to the nerve in this region or it could be related to an under-diagnosis of tarsal tunnel as a primary problem.
The pain associated with tarsal tunnel is always noted to be worse as the day progresses whereas the pain associated with plantar fascitis is worse with initial rising.
Diagnosis of tarsal tunnel syndrome is “clinical”, meaning a good history and exam performed by your physician will help establish this diagnosis. Additional studies including electrophysiologic studies in the form of nerve conduction studies can be performed to help support the diagnosis. Sensory nerve conduction studies provide some of the greatest electrophysiologic proof of tarsal tunnel syndrome. Motor nerve conduction studies are often performed by neurologist and are often found to be negative and can create confusion between patient and physician with regard to the accuracy of the “clinical” diagnosis. If soft tissue masses are noted to be palpably present on exam an MRI can help determine what soft tissue pathology may be of concern.
Treatment for tarsal tunnel is very similar to the treatment protocols followed for plantar fascitis:
 Supportive shoe and orthotic use to stabilize the rearfoot position if there is abnormal foot pronation is generally used to take abnormal stresses off of the nerve.
Supportive shoe and orthotic use to stabilize the rearfoot position if there is abnormal foot pronation is generally used to take abnormal stresses off of the nerve.

Custom or over the counter orthotic to decrease abnormal foot pronation used in conjunction with the supportive shoe

Short term walking cast immobilization (CAM Boot)
Anti-inflammatory agents including ice, non steroidal anti-inflammatory (NSAIDS), including ibuprofen or naproxen, and the selective use of cortisone injections into the region of the tarsal tunnel can be used.
ICE twice daily
Physical therapy
The pain associated with tarsal tunnel syndrome is difficult to manage. If symptoms progress despite aggressive conservative measures surgery may be indicated. It is important to note that surgery as a treatment option should not be ignored or deferred if conservative attempts at pain relief have not been successful. The pain associated with tarsal tunnel can become chronic if the nerve is not surgically decompressed.
The surgical care for tarsal tunnel syndrome is performed on an outpatient surgical basis and generally involves the surgical release of any tight soft tissues around the nerve extending from the ankle region and into the foot through the anatomical path of the nerve through the porta pedis. The most important portion of the surgical care involves the dissection and release of the muscle fascia to the abductor hallucis brevis at the porta pedis. The muscle fascia is the fibrous tissue that surrounds and encapsulates the muscle tissue. By releasing the tight soft tissues following the course of the nerve the area is decompressed which will allow the nerve in the post operative state to function normally.
The results of surgical decompression of the tarsal tunnel are mixed with surgical relief of pain ranging from 60-95%. This broad range of successful outcomes may be related to the surgical technique used for the surgical decompression. Overzealous dissection of the fatty tissue surrounding the involved posterior tibial nerve may negatively impact surgical outcomes.
Post surgical care includes non-weight-bearing cast immobilization for three weeks with advancement to a removable cast brace for an additional three weeks prior to advancement into comfortable supportive shoe gear. Formal physical therapy begins at three weeks postoperatively and includes aggressive soft tissue mobilization around the scar tissue to decrease scarring in the region.
Improvement of any nerve dysfunction generally will be noted initially after surgery but can continue to improve up to one year post operatively. At the three month juncture post operatively patients should have resumed near normal return to activity.
Establishing the diagnosis of tarsal tunnel is a critical first step in the recovery process. Symptoms can sometimes be ill defined but observation of the pain symptoms as well as the clinical reproduction of pain at the tarsal tunnel region help to confirm the diagnosis. Although conservative therapy should be approached aggressively there are no reported studies showing success rates of conservative outcomes. If surgical release is indicated, complete release of the posterior tibial nerve course in this region must be performed to ensure successful pain relief outcome.
Related Articles
-
Effect of foot and ankle position on tarsal tunnel compartment volume.Read Article »
- Tarsal tunnel syndrome: a compression neuropathy involving four distinct tunnels.
Read Article »- Peripheral nerve entrapments.
Read Article »Related Products
-
 ASICS - 2150 - Womens
ASICS - 2150 - WomensA running shoe built for the moderate to excessive over-pronator who requires a combination of cushioning and reinforced stability.
Schedule an Appointment

Please call 805.543.7788 for San Luis Obispo, 805.434.2009 for Templeton, or email us to request an appointment.
- Tarsal tunnel syndrome: a compression neuropathy involving four distinct tunnels.